
Bunions in 2025: Evidence, Options, and Why Minimally Invasive Lapidus Leads the Pack

TLDR
Bunions are a common and often progressive deformity, affecting up to one in three older adults.¹ ² Conservative care can reduce pain and improve shoe comfort but does not reliably reverse bone alignment in adults.⁶ ⁷ I recommend footwear changes (Topo being my go-to brand) and other nonoperative measures for symptom relief in early or mild cases. For patients who need surgery, I primarily perform minimally invasive Lapidus-based procedures such as Treace Lapiplasty and Stryker PROstep MIS Lapidus — allowing most to walk in a boot the same day.⁹ ¹⁰ ¹² ¹³ ¹⁴ Other options such as distal chevron, scarf, and Akin osteotomies remain valuable in select patients. For pediatric bunions, conservative care, growth monitoring, and careful surgical timing are key. Bunion splints? I never recommend them.
What is a Bunion?
A bunion, or hallux valgus, is a three-dimensional deformity involving medial deviation of the first metatarsal, lateral deviation and pronation of the hallux, and instability at the first tarsometatarsal (TMT) joint.⁵ The triplanar nature explains why purely two-dimensional corrections often relapse — true correction must address all planes and the apex of deformity.⁵ ⁹
Epidemiology: How Common Are Bunions?
Bunions are one of the most common forefoot deformities worldwide. In adults, the prevalence is about 23%, rising to 36% in older populations.¹ ² Women are roughly twice as likely to develop bunions, likely due to footwear choices, ligamentous laxity, and genetic predisposition.¹
In some populations, especially those with a cultural tendency toward narrow or high-heeled footwear, prevalence rates climb even higher.¹ ² A recent meta-analysis also confirmed that bunions are more common in those with flatfoot, ligamentous laxity, and a family history of hallux valgus.²

This condition is not just cosmetic. It is associated with pain, decreased walking efficiency, increased fall risk in elderly patients, and reduced quality of life.³
Common companions: Pain under the big toe joint is often sesamoiditis. Numbness between the lesser toes can be Morton’s neuroma.
Pediatric Bunions: A Different Consideration
Juvenile or adolescent hallux valgus behaves differently from adult bunions. The deformity is often more flexible but progresses with growth, especially if there is ligamentous laxity or flatfoot.
Signs parents may notice include:
Shoe fit problems
Overlapping toes
Visible deviation of the big toe, even without pain
Pain is not always the first symptom in children, which is why careful monitoring is important.
Management tips for pediatric bunions:
Conservative care first: Shoes with wide toe boxes (Topo works well here too), orthotics for underlying flatfoot, and activity modification.
Avoid splints for “correction”: No evidence for durable benefit, and they may cause compliance issues.
Delay surgery until skeletal maturity unless symptoms and deformity are severe. Early surgery carries a higher recurrence risk.²⁰
Education is key: Families should understand progression and realistic expectations for long-term management.
Conservative Care: Relief, Not Cure
Nonoperative care aims for symptom relief, better shoe fit, and slower progression — not reversal of deformity in adults.⁶ ⁷
What I recommend
Shoes: Topo is my first choice due to its combination of a wide toe box, secure midfoot, and mild rocker sole. Altra is an excellent alternative with zero-drop and a foot-shaped toe box, especially for casual wear. HOKA Bondi and Skyline provide rocker-sole forefoot offloading for active patients. Brooks Ghost Max 3 and New Balance Fresh Foam More are strong cushioned trainers with roomy toe boxes that have tested well in bunion comfort reviews.⁶ ²² Several studies have shown that footwear with adequate toe box width and cushioning can significantly reduce bunion-related pain and improve gait efficiency.²²
Orthoses: Custom or prefabricated OTC like Powersteps with a Morton’s extension to protect the joint, improve comfort, redistribute plantar pressures, and address coexisting flatfoot or metatarsalgia.
Activity modification: Reducing activities that exacerbate forefoot loading.
NSAIDs and icing as needed for inflammation control.
What I don’t recommend
Bunion splints: While they may temporarily reduce pain or toe overlap in a shoe, they do not change bone position long-term. Evidence shows no lasting structural benefit in adults.⁶ ⁷
Shoe comfort and mechanics: If arch or heel pain limits your walks, compare with plantar fasciitis. Nail edge tenderness from crowding fits the pattern in ingrown toenails.
When to Consider Surgery
I consider surgery when patients have:
Persistent pain despite appropriate conservative care
Shoe intolerance or inability to participate in desired activities
Progressive deformity with functional changes (transfer lesions, hammertoe development)⁴ ²⁰
Surgical decision-making is based on symptoms, functional goals, and deformity type — not solely on radiographic angles.⁴
Surgical Options: Why I Favor Lapidus-Based Procedures
The Lapidus procedure fuses the first TMT joint (the joint BEHIND where you see the bunion sticking out), correcting deformity at its origin and in all three planes.⁵ ⁹ This is especially valuable for:
Severe angular deviation
Hypermobility of the first ray
Recurrent bunions after distal osteotomy
Younger patient’s and Pediatric patients that need a time-tested surgical technique with low recurrence rates
Modern fixation allows protected early weight bearing, which I’ve incorporated into my protocol — most patients walk in a boot the same day.¹² ¹³ ¹⁴
Instrumented triplanar correction at the TMT joint with biplanar plating.⁹ ¹⁰ ¹¹
Reported fusion rates ~99% with low recurrence.¹¹
Early boot walking is often possible in 7–10 days in studies; in my protocol, it is usually same day for healthy adults.
A version of the Lapiplasty called the Adductoplasty
While this specific technique is for SEVERE bunions, it shows the power of the lapidus technique using the Lapiplasty hardware
True minimally invasive construct allowing triplanar correction through a few small 1-2 stitch incisions.¹⁶
Early results indicate it works well with my early boot protocol, as with most minimally invasive techniques the literature is fairly new and emerging. However, anecdotally my fusion and success rates are equally as high as my open techniques.

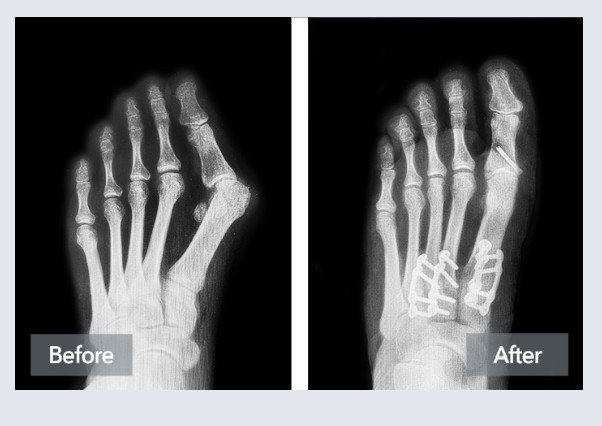
Stryker ProStep MIS hardware, also pictured is the Stryker MIS tailors bunion nail
This patient was allowed to bear weight on the foot the day of surgery in a walking boot
Early Weight Bearing: The Protocol Advantage
Multiple studies support that with stable fixation, early protected weight bearing does not compromise fusion or correction.¹² ¹³ ¹⁴ Benefits include:
Improved patient confidence
Maintenance of calf mobility
Reduced risk of deconditioning
Shorter time to functional independence
How MIS Compares to Open Surgery
Systematic reviews and meta-analyses show that MIS and open approaches can achieve similar radiographic correction.⁵ ¹⁸ MIS often results in:
Faster early recovery
Lower wound complication rates
Higher early patient satisfaction
However, recurrence prevention depends more on achieving true triplanar correction and stable fixation than on incision size.³
A 2024 comparative review found that Lapiplasty had significantly lower recurrence rates and higher satisfaction scores at 2 years than scarf or chevron osteotomies in moderate-to-severe deformities.²² This aligns with the concept that correcting at the deformity’s apex (the TMT joint) improves durability.
Surgical Options: Beyond the Lapidus
While I favor Lapidus-based procedures for moderate-to-severe or hypermobile bunions, several other surgical techniques have merit and a place in my bunion correction arsenal
| Procedure | Best For | Key Points | Drawbacks |
|---|---|---|---|
| Distal Chevron Osteotomy | Mild deformity, younger patients | Quick recovery, good pain relief | Limited correction power, not for severe deformities |
| Scarf Osteotomy | Mild-to-moderate | Allows more correction than chevron, stable fixation | Larger incision, less triplanar correction |
| Akin Osteotomy | Often adjunctive | Corrects hallux valgus interphalangeus | Rarely standalone |
| Proximal Metatarsal Osteotomies | Moderate-to-severe without hypermobility | Greater correction than distal | Longer recovery, higher recurrence if instability unaddressed |
| MTP Joint Arthrodesis | Arthritic, salvage cases | Eliminates pain in end-stage arthritis | Loss of joint motion |
Risks & Recurrence
All bunion surgeries carry risks — nonunion, infection, nerve irritation, stiffness, hardware issues, and recurrence.³ Recurrence rates are lowest when TMT instability is addressed and sesamoid position is restored. ³ ⁹ ¹¹
Bottom Line for Adults
Try symptom management first: footwear, orthotics, and activity adjustments.
Skip bunion splints for correction — they won’t create lasting structural change.
If surgery is indicated, choose the procedure that best addresses your deformity in three planes and secures the correction well enough to allow safe, early return to walking.
Bottom Line for Pediatrics
Focus on comfort and shoe fit.
Monitor for progression, especially during growth spurts.
Delay surgery until skeletal maturity unless symptoms are severe.
Use orthotics if flatfoot is present.
Avoid splints — no lasting benefit and potential compliance issues.
Bunion FAQ
Do bunion splints fix the bone?
No. They may offer comfort but do not realign the first metatarsal. Alignment changes require surgery when symptoms and function demand it.¹
When is surgery reasonable?
When pain or shoe conflict limits life despite shoe changes, orthoses, and activity adjustments. Imaging and exam guide the procedure choice.¹
Will shoes alone stop progression?
Shoes can improve comfort and reduce symptoms. Progression depends on anatomy, ligament laxity, and load.¹
¹ References align with the main article’s citations from peer‑reviewed sources including JFAS, APMA, and AOFAS.
🦶 Recommended Products for Bunions
These items are listed for education and reference only. They are not a substitute for medical advice. Please see your podiatrist for specific recommendations. I may receive a commission if you purchase through these links, at no additional cost to you.
👟 Shoes
- Topo Ultraventure 4 – Trail shoe with wide toe box to reduce bunion irritation
- Topo Atmos – Maximalist shoe with roomy forefoot
- Altra Torin 8 – Zero-drop shoe with naturally wide forefoot fit
🦾 Orthotics
- Powerstep Pinnacle Maxx – Helps control pronation contributing to bunion pressure
References
Nix S, Smith M, Vicenzino B. Prevalence of hallux valgus in the general population. J Foot Ankle Res. 2010;3:21.
Cai Y, Song Y, He M, et al. Global prevalence and incidence of hallux valgus. J Foot Ankle Res. 2023;16:64.
Barg A, Harmer JR, Presson AP, et al. Unfavorable outcomes following surgical treatment of hallux valgus deformity. J Bone Joint Surg Am. 2018;100(18):e119.
Wagner E, Wagner P, Ortiz C. Metatarsal pronation in hallux valgus deformity. JAAOS Glob Res Rev. 2020;4(6):e20.00094.
Hurn SE, Vicenzino B, Smith MD. Non-surgical interventions for hallux valgus. Arthritis Care Res. 2021;73(9):1270-1281.
Glasoe WM, Loper A, Rauh MJ. Effects of foot orthoses and taping on hallux valgus pain and function. J Prosthet Orthot. 2022;34(1):58-69.
Torkki M, Malmivaara A, Seitsalo S, et al. Surgery versus orthosis versus watchful waiting for hallux valgus. JAMA. 2001;285(19):2474-2480.
Ray JJ, et al. Multicenter early radiographic outcomes of triplanar first tarsometatarsal arthrodesis with early weightbearing. Foot Ankle Int. 2019;40(8):955-960.
Dayton P, et al. Early weightbearing after triplanar first tarsometatarsal arthrodesis. J Foot Ankle Surg. 2019;58(3):427-433.
Prissel MA, Hyer CF, Grady JF, et al. A multicenter retrospective study of early weightbearing for modified Lapidus arthrodesis. J Foot Ankle Surg. 2016;55(2):226-229.
King CM, Richey J, Patel S, Collman DR. Modified Lapidus arthrodesis with early weightbearing in 136 patients. J Foot Ankle Surg. 2015;54(1):69-75.
Blitz NM, et al. Early weightbearing after modified Lapidus arthrodesis. J Foot Ankle Surg. 2010;49(3):221-226.
Crowell A, Van JC, Meyr AJ. Early weightbearing after first metatarsal–medial cuneiform arthrodesis: systematic review. J Foot Ankle Surg. 2018;57(6):1204-1206.
Ji L, Wang K, Ding S, et al. Minimally invasive versus open surgery for hallux valgus. Front Surg. 2022;9:843410.
Stryker. PROstep MIS Lapidus operative technique guide. 2023.
Harb Z, Kokkinakis M, Ismail H, Spence G. Adolescent hallux valgus: systematic review of outcomes following surgery. J Child Orthop. 2015;9(2):105-112.
Menz HB, Akele BD, Whittaker GA, et al. Effectiveness of footwear and foot orthoses in reducing plantar pressure in women with hallux valgus. Gait Posture. 2024;109:199-206.