
Intoeing In Children: What Is Normal, What Is Not, And What Actually Helps
Parents worry about intoeing because it is so visible and so common, especially in toddlers and early grade school kids. The good news is that most children outgrow it without special shoes or braces, and the data behind that statement is strong.¹ ² ³

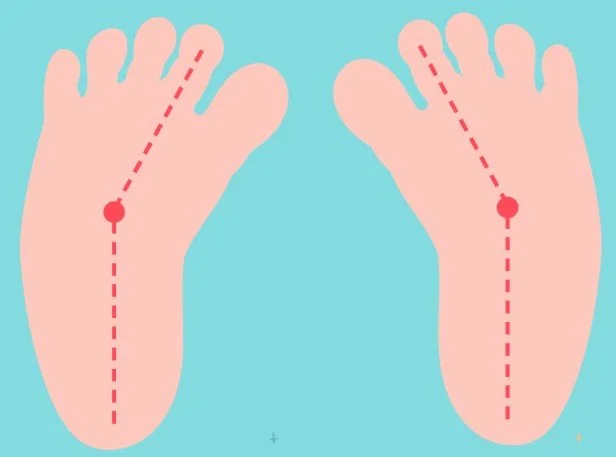
Pediatric Intoe
The common foot issue that brings much more worry than probably warranted, read below to understand why
The big three causes of intoeing
Most intoeing comes from one of three age linked patterns. Metatarsus adductus is a curved in forefoot that shows up in infancy. Internal tibial torsion is an inward twist of the shin that becomes obvious in toddlers. Femoral anteversion is an inward twist of the thigh that often appears after age three and pairs with W sitting.¹ ² ³ ⁴
These patterns follow predictable timelines. Metatarsus adductus dominates in the first year. Internal tibial torsion is common through about age three. Femoral anteversion is most noticeable from early school years through about age eight to ten as the hips gradually unwind.¹ ² ³
As kids grow: Family foot shape can influence adult issues like bunions. Later teen or adult heel pain has a different workup, which I cover in plantar fasciitis.
Natural history favors patience
The headline is simple. Typical internal tibial torsion improves on its own before school age, and femoral anteversion steadily normalizes during the grade school years. Special shoes, bars, or twister cables do not speed correction. Multiple guidelines from AAOS, POSNA, and primary care reviews agree on observation with periodic measurement for healthy children who are active and pain free.¹ ² ³ ⁴
Observation is not doing nothing. We document a torsional profile in clinic that includes hip rotation, the thigh foot angle, and the foot progression angle while walking. This places the child on the expected curve and lets families see improvement over time.¹ ³
Parent blip. If your kid runs hard at recess and sleeps well, you are already winning.¹
What helps and what does not
Helpful approaches include education, time, and letting kids play to comfort. There is no credible evidence that routine bracing or special shoes change bone torsion in idiopathic internal tibial torsion or femoral anteversion.¹ ² ³ ⁴
Metatarsus adductus is the one early exception. A flexible forefoot usually straightens without intervention. A rigid curve that does not correct may benefit from serial casting or an orthotic program during infancy, with randomized data showing at least equivalent outcomes and lower cost for an orthosis program in some cohorts.² ⁵ ⁶
Forefoot Angle of Metadductus
Flexible deformities will usually correct with time to the straight line, rigid may need more help
When pediatric insoles and physical therapy actually help
Truth first. Insoles and therapy do not untwist bones. They can reduce pain, improve balance, and make day to day life easier while nature does the long work. Use them for comfort and function, not as a promise to change torsion.¹ ² ³
Symptomatic flexible flatfoot with pain or easy fatigue
Systematic review data in children and adults shows mixed structural change but supports symptom relief in selected patients, especially for pain and activity tolerance. For many families that is the outcome that matters.⁷ ⁸ Parent tip: If the goal is fewer end of day complaints, an insole trial is reasonable.⁷ ⁸
Calcaneal apophysitis also called Sever disease
Randomized data suggests both heel lifts and custom orthoses improve pain, with some trials favoring custom orthoses for short term relief. Expectations matter because most kids improve within a few months regardless.⁹ ¹⁰
Frequent tripping where fall risk is the main issue
The evidence base is small and of modest quality, but gait plate style insoles or wedged insoles may slightly increase the foot progression angle and reduce tripping in the short term. Use as a practical safety aid, not as a cure.¹¹ ¹²
Neuromuscular conditions
Children with neuromuscular diagnoses are a different category. Targeted orthoses or rotational systems may help alignment and efficiency when paired with a rehabilitation plan. This sits outside typical idiopathic intoeing and warrants specialist management.¹ ²
Physical therapy focus
For kids who are clumsy, avoid playground challenges, or meet criteria for coordination difficulties, short blocks of task specific balance, hopping and landing drills, hip external rotator and abductor strength, foot intrinsic activation, and calf mobility can improve function and confidence. Therapy complements insoles for painful flatfoot and supports a safe return to play.¹ ³
How to run a practical insole and therapy trial
In clinic, I start with a prefabricated orthotic device that supports the arch and cups the heel. For heel pain, a deep heel cup or small lift is reasonable. Reassess in six to eight weeks. Continue if activity goes up and complaints go down. Stop if there is no meaningful change. Pair with a four to six week home centered program built around balance progressions and age appropriate plyometrics.⁷ ⁹ ¹¹ Custom orthotic devices can be used for more advanced control of the foot but aren’t always needed.

Custom Gait Plate
Built exactly to your child’s foot, used to help the foot align back to midline while wearing the orthotic and shoes
Foot care basics for families: If a toenail becomes tender or red, review home and office care for ingrown toenails. Thick or discolored nails are explained in toenail fungus.
Red flags that should prompt earlier Podiatry referral
Painful or progressive deformity, clear asymmetry, rigid foot that does not correct, limp, neurologic signs, trauma or infection history, developmental delay, or clinical concern for clubfoot deserve a closer look and often imaging.¹ ³ ⁴
How I evaluate this in clinic
History covers: age of onset, tripping or pain, family pattern, and seating habits. Examination measures hip rotation, thigh foot angle, heel bisector for metatarsus adductus, and foot progression angle during gait. Imaging is rarely needed for typical cases. The goal is to identify the pattern, place it on the normal timeline, and track change with growth.¹ ³
Bottom line for families and referring clinicians
Most intoeing in healthy kids is a normal developmental variation that improves with growth. Education on the condition, activity level to comfort, and periodic measurement are the right plan for the majority of kiddos. Use casting or an orthosis program for rigid metatarsus adductus in infancy. Consider surgery only for older children with severe persistent torsion that clearly impairs function. Be skeptical of devices that claim to straighten a child faster. The data does not support those promises.¹ ² ³ ⁴ ⁵
Products Actually Used or Recommended In My Practice for Pediatric Intoeing:
These items are listed for education purposes and references only, not to replace seeing your provider for specific recommendations, I may receive commission for any items purchased.
Do not blindly purchase products online for this condition. Please see your podiatrist or pediatric orthopedist for personalized recommendations. As noted earlier, the underlying cause of intoeing varies from child to child — and so does the best approach, whether that means treatment, monitoring, or no intervention at all.
Pediatric Intoeing FAQ
Do most kids outgrow intoeing?
Yes. Most children improve naturally as bones and gait mature. Reassurance and simple shoe tips go a long way.¹
Do braces or special shoes speed it up?
Current evidence does not support routine bracing for typical flexible intoeing. Guidance and monitoring are preferred.¹
When should we see a specialist?
See a specialist if there is pain, tripping that limits play, asymmetry, rigid deformity, or regression after prior improvement.¹
¹ References align with the main article’s citations from peer‑reviewed sources including JFAS, APMA, and AOFAS.
👨👩👧 Parent Resources for Pediatric Intoeing
Intoeing is one of the most common concerns I hear from parents. The good news is that most children outgrow it naturally without braces, special shoes, or surgery. Here are trusted references and tips for families:
📚 Helpful References
- American Academy of Orthopaedic Surgeons – Intoeing Overview
References
Rerucha CM, Dickison C, Baird DC. Lower extremity abnormalities in children. American Family Physician. 2017
Pediatric Orthopaedic Society of North America. Torsional problems, study guide.²
American Academy of Orthopaedic Surgeons. OrthoInfo, Intoeing. Last reviewed 2024.
Talley W, Blackhurst DW. Managing intoeing in children. American Family Physician. 2011.
POSNA Study Guide. Metatarsus adductus, with randomized comparison of casting versus orthosis, Herzenberg 2014.
Herzenberg JE, Lamm BM, Corwyn C, et al. Resistant metatarsus adductus, randomized trial of casting versus orthosis. J Pediatr Orthop B. 2014.
Oerlemans LNT, et al. Foot orthoses for flexible flatfeet in children and adults, systematic review and meta analysis. BMC Musculoskelet Disord. 2023.
Oerlemans LNT, et al. PubMed record for the same systematic review. 2023
Alfaro Santafé J, et al. Custom orthoses versus heel lifts for calcaneal apophysitis, randomized trial. Children. 2021.
Alfaro Santafé J, PubMed abstract. 2021.
Uden H, Kumar S. Non surgical management of pediatric intoed gait, systematic review. 2012.
Uden H, PubMed record for the same review. 2012.