
Sesamoiditis: Big Pain From Little Bones Under the Great Toe
If you feel like you are constantly stepping on a pebble right under your big toe joint, you may be dealing with sesamoiditis. The sesamoids are two tiny bones under the ball of the foot that act like little kneecaps for your big toe. When they become irritated, bruised, or fractured, the pain can make even standing a challenge.
Most people never know these bones exist. The few who do usually learn the hard way—through pain.
What Are Sesamoids?
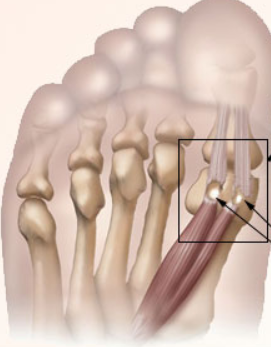
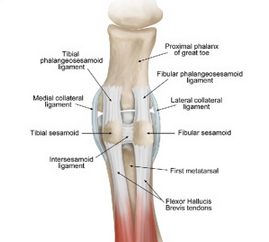
Sesamoids are two small bones (about the size of jelly beans) that sit beneath your big toe joint inside the tendons of the flexor hallucis brevis muscle. Together with surrounding ligaments, they form the sesamoid apparatus.
Tibial sesamoid: sits closer to the inside edge of your foot
Fibular sesamoid: sits closer to your second toe
Their job is to:
Act as pulleys for tendons, making push-off more efficient
Absorb shock when walking, running, or jumping
Provide stability to the first metatarsophalangeal (MTP) joint¹
These bones carry a disproportionate share of pressure, especially in athletes and dancers.
Why this pain happens: Big toe alignment changes from bunions can push extra load on the sesamoids. Calf tightness and tendon overload from Achilles tendinopathy can add stress too.
Symptoms of Sesamoiditis
Common signs include:
Pain: sharp, aching, or burning under the big toe joint, worse barefoot or in thin shoes
Swelling: localized puffiness compared to the other foot
Bruising: sometimes seen after trauma or early stress injury
Stiffness: painful and reduced upward motion of the big toe
Tenderness to touch: pain directly under the first metatarsal head²
In severe cases, walking may be nearly impossible.
Causes of Sesamoid Pain
Overuse
The most common cause. Seen in runners, dancers, basketball players, and people who spend long hours on hard floors. Repetitive stress gradually overloads the sesamoids. If ignored, this can progress to a stress fracture³.

Trauma
Landing hard on the ball of the foot, dropping something heavy, or slamming the foot in a car accident can bruise or fracture the sesamoids immediately.
Turf Toe
A specific ligament injury where the big toe is forcibly bent upward. Common in football but possible in any sport requiring sudden push-off. Turf toe damages the ligaments around the sesamoids and may also fracture the bones⁴.

Foot Structure
Certain foot types are at higher risk:
High arches (more pressure on the ball of the foot)
Bunions (which shift pressure toward the sesamoids)
People with naturally larger sesamoids or first metatarsal anatomy that predisposes overload⁵
Conservative Treatment Options
Most patients improve without surgery.
1. Activity Modification
Rest from high-impact exercise
Replace running/jumping with swimming, rowing, or cycling
Avoid walking barefoot on hard surfaces
2. Footwear Changes
Supportive athletic shoes with stiff soles reduce big toe motion
Avoid high heels and flexible minimalist shoes that overload the forefoot
3. Padding and Orthotics
Dancer’s pad: offloads weight away from sesamoids while allowing normal walking
Custom orthotics: long-term solution for recurrent pain or underlying foot structure issues⁶

4. Immobilization
Walking boot or stiff surgical shoe limits motion
Crutches may be recommended early for severe cases
5. Physical Therapy and Dry Needling
Therapy focuses on improving foot mechanics, strengthening, and restoring motion. Dry needling and manual therapy have shown benefit in reducing myofascial pain and improving mobility around the sesamoid complex⁷.
6. Anti-inflammatory Measures
Ice massage after activity
Short courses of oral NSAIDs if appropriate
Rarely, a corticosteroid injection may be used, though many surgeons avoid injecting directly into sesamoids because of risk of bone weakening⁸
Surgical Options
Reserved for fractures or chronic pain that fails conservative care.
Sesamoidectomy: removal of one sesamoid bone. Provides reliable pain relief but carries a small long-term risk of bunion development⁹.
Percutaneous screw fixation: used for fresh fractures in two large pieces. Healing requires 4–6 weeks of limited weightbearing.
Open fixation with bone graft: for chronic fractures in multiple pieces. Bone graft helps stimulate healing. Requires strict offloading for 6–8 weeks.

Next steps: If arch or heel symptoms are louder in the morning, skim my plantar fasciitis guide. Numbness or burning between toes points to Morton’s neuroma.
Recovery Timeline
Mild inflammation: 2–6 weeks with rest, padding, and shoe changes
Stress fractures/turf toe: 6–12 weeks in a boot or orthotic device
Surgery:
Sesamoidectomy: walking in a surgical shoe right away, stitches out at 2 weeks, return to normal shoes in 3–4 weeks
Screw fixation/graft: 2–3 months before return to sport, sometimes longer for high-impact athletes
Prevention Strategies
Replace worn-out athletic shoes every 300–500 miles
Use pads or orthotics if you’ve had sesamoid issues before
Cross-train to reduce repetitive pounding
Warm up and stretch before intense activity
Address bunions or foot alignment problems early
Pediatric and Young Athlete Considerations
Children and teens in ballet, cheer, or gymnastics are particularly vulnerable. Their bones are not fully hardened, making them more susceptible to stress injuries. Early intervention prevents long-term problems. Parents should never ignore persistent pain under the big toe joint in kids. An X-ray or MRI may be needed to rule out stress fracture.
Conclusion
Sesamoiditis may involve the smallest bones in your foot, but the pain can be one of the biggest. The good news is that most cases heal with rest, shoe modifications, and offloading pads. For stubborn injuries or fractures, surgical options are available with good long-term outcomes.
Taking your sesamoid pain seriously now can prevent bigger problems later and get you back to walking, running, or dancing pain-free.
Sesamoiditis FAQ
Why does pain sit under the big toe joint?
The sesamoids act like tiny kneecaps for the big toe. They bear load during push off and can get irritated with forefoot pressure and calf tightness.¹
Do I need to stop activity?
Usually you modify rather than stop. Offload the forefoot, adjust shoes, and start a graded return as pain settles.¹
When is surgery considered?
Only after a focused period of offloading and rehab fails or when imaging shows a fracture or chronic nonunion with persistent pain.¹
¹ References align with the main article’s citations from peer‑reviewed sources including JFAS, APMA, and AOFAS.
🦶 Recommended Products for Sesamoiditis
These items are listed for education and reference only. They are not a substitute for medical advice. Please see your podiatrist for specific recommendations. I may receive a commission if you purchase through these links, at no additional cost to you.
👟 Shoes
- Topo Ultraventure 4 – Cushioned trail shoe with wide toe box
- Topo Atmos – Maximalist shoe with roomy forefoot
- Altra Torin 8 – Zero-drop shoe for natural forefoot loading
🦾 Orthotics
- Powerstep Mortons Extension – Designed to offload sesamoids and first toe joint
🧰 Rehab Tools
- Metatarsal Pads – Stick-on pads to relieve pressure under the big toe joint
References
Pretterklieber ML. Anatomy and biomechanics of the first ray. Foot Ankle Clin. 2001;6(1):1-20.
Faltus J, et al. Clinical features and treatment of sesamoid disorders. Curr Rev Musculoskelet Med. 2017;10(1):85-93.
Saxena A, et al. Return to activity after sesamoid stress fractures. J Foot Ankle Surg. 2003;42(6):355-358.
Clanton TO, et al. Turf toe injury: anatomy, diagnosis, and treatment. Sports Health. 2012;4(6):537-544.
Bouche RT, Heit EJ. Sesamoid disorders of the first metatarsophalangeal joint. J Am Podiatr Med Assoc. 2008;98(6):438-448.
American Podiatric Medical Association. Sesamoid Injuries. Accessed 2025.
Brady S, et al. Dry needling for myofascial pain. J Orthop Sports Phys Ther. 2014;44(9):623-634.
Kane JM, et al. Corticosteroid injections in foot and ankle conditions. Foot Ankle Int. 2015;36(9):1059-1066.
Richardson EG, et al. Sesamoidectomy for painful hallux sesamoid disorders. Foot Ankle Int. 1999;20(8):464-469.